Muhammad Ali Fauzi
Department of Information Security
and Communication Technology
Norwegian University
of Science and Technology (NTNU)
Gjøvik, Norway
muhammad.a.fauzi@ntnu.no
Prosper Yeng
Department of Information Security
and Communication Technology
Norwegian University
of Science and Technology (NTNU)
Gjøvik, Norway
prosper.yeng@ntnu.no
Bian Yang
Department of Information Security
and Communication Technology
Norwegian University
of Science and Technology (NTNU)
Gjøvik, Norway
bian.yang@ntnu.no
Dita Rachmayani
Department of Psychology
Universitas Brawijaya
Malang, Indoneisa
dh33ta@ub.ac.id
Peter Nimbe
Department of Computer Science and Informatics
University of Energy and Natural Resources
Sunyani, Ghana
peter.nimbe@uenr.edu.gh
Abstract
This study aims to investigate the relationship between stress levels among hospital staff and their risky cybersecurity practices. A web-based survey was conducted with a
sample of 353 hospital staff from Ghana, Norway, and Indonesia.
The results indicate a statistically significant positive correlation
between the stress levels of hospital staff and their engagement in
unsafe cybersecurity practices (r = 0.201, p < 0.01). Specifically,
the study finds that staff members’ inclination to click on
links from unknown sources is the cybersecurity practice most
strongly influenced by stress levels. The study did not observe
any significant differences in cybersecurity practices based on
gender, age, job, position level, or work experience. However,
it does highlight notable differences in cybersecurity practices
across countries, with Norwegian hospital staff exhibiting better
cybersecurity practices than their counterparts from Ghana and
Indonesia.
Index Terms—Stress, Cybersecurity Practice, Demographic,
Healthcare, Hospital, Norway, Ghana, Indonesia, Correlation.
Introduction
Electronic health records (EHRs), telemedicine, and remote
patient monitoring systems have all been adopted in recent
years, undergoing a considerable digital transition in the
healthcare sector. Even though these technological developments have improved patient outcomes and the quality of
treatment, they have also presented new cybersecurity threats
to hospitals and their workers. Due to the enormous volumes of sensitive patient data that are electronically kept and
exchanged, the healthcare sector is especially susceptible to
cyber-attacks [1]. Data breaches, financial losses, reputational
harm, and, most crucially, jeopardized patient care are all
possible outcomes of these attacks [2]
It is generally known that human factors are one of the
major causes of cybersecurity breaches. Human error may
compromise even the most sophisticated technological security
measures [3], [4]. For instance, according to a recent Verizon
research, humans were involved in 82% of all data leaks
[1]. Therefore, many prior studies focused on understanding
how the human factor can affect cybersecurity practices and
identify the factors that affect cybersecurity practices [5]–[9].
Stress is one of the human factors that can affect cybersecurity practices. Stress can lead to lapses in judgment,
increased impulsivity, and a reduced ability to make rational
decisions [10]–[12]. In the context of cybersecurity, stress may
lead to unsafe cybersecurity practices, such as clicking on
suspicious links or responding to phishing emails. Hence, it is
essential to understand the impact of stress on cybersecurity
practices. However, only a few studies focused on this topic,
especially in the healthcare setting. Moreover, most of the
studies were conducted in developed countries. McCormac et
al. [13] analyzed the effect of job stress on information security
awareness among company workers in Australia while Fordyce
et al. [14] investigated the effect of stress on password choice
among students in United Kindom. There is no study on this
topic conducted in developing countries.
This study aims to investigate the relationship between hospital staff stress levels and cybersecurity practices in Norway
and two developing countries, Ghana and Indonesia. This
study follows the hypothesis that hospital workers with higher
stress levels engage in riskier security practices. Additionally,
we will also compare the cybersecurity practices between these three countries and examine the relationship between
demographic variables and cybersecurity practices. By examining this relationship, this study can contribute to the existing
literature on cybersecurity in the healthcare industry and
provide insights for hospitals to improve their cybersecurity
practices.
Materials and methods
Research approach
This study’s primary objective was to examine the relationship between stress levels and cybersecurity practices among
hospital staff. The research approach is outlined in Figure 1.
To achieve this objective, an online survey developed using
Nettskjema was utilized to collect data on healthcare staff’s
demographic details, stress levels, and cybersecurity practices
within the past month. Nettskjema is an online survey platform
that places a high priority on data privacy and security run by
the University of Oslo. The survey was composed in English
for participants from Ghana, Norwegian for participants from
Norway, and Indonesian for participants from Indonesia. The
participants’ stress levels and risky cybersecurity practices
were assessed using the Perceived Stress Scale (PSS) and
Hospital Staff’s Risky Cybersecurity Practices Scale (HSRCPS), respectively. Additionally, the questionnaire included
an attention-checking question to guarantee the response’s
quality. Hospital employees from three hospitals in Ghana, a
hospital in Norway, and a hospital from Indonesia were invited
to participate in the study. All participants provided their
written consent electronically, and the surveys’ completion and
analysis were completely anonymous.
Perceived Stress Scale (PSS)
The Perceived Stress Scale (PSS) is a self-report survey
used to measure individuals’ perceptions of stress. It uses a
5-point Likert scale to assess the frequency of thoughts and
feelings connected to stress during the previous month. PSS
assesses the subjective experience of stress rather than specific
stressors. PSS has three variations: PSS-14, PSS-10, and PSS4, with PSS-10 having superior psychometric properties than
the others [15]. PSS has been translated and validated in
many languages, indicating its cross-cultural applicability. This
study will use the Norwegian language version of PSS. In
this study, we used the original English version of PSS-10 for
participants from Ghana. Meanwhile, the Indonesian version
by Pin [16] was used for Indonesian participants and the
Norwegian version translated by CheckWare AS [17] was
employed for Norwegian participants.
Hospital Staff ’s Risky Cybersecurity Practices Scale (HSRCPS)
The Hospital Staff’s Risky Cybersecurity Practices Scale
(HS-RCPS) was developed to evaluate hospital staff’s cybersecurity practices based on the Human Aspects of Information
Security Questionnaire (HAIS-Q) and the Security Behavior
Intentions Scale (SeBIS). The scale was tailored specifically
to measure the cybersecurity practices of healthcare workers based on feedback from interviews with 36 healthcare employees and cybersecurity professionals from various universities
and hospitals in Ghana, Indonesia, and Norway. The scale
consists of 12 items with a possible total score ranging from
0 to 48. Higher scores indicate riskier cybersecurity practices
over the past month. Participants were asked to rate their
engagement in specific cybersecurity practices using a scale
of 0 to 4 (”disagree” to ”agree”). This scale is available in
English, Norwegian, and Indonesian versions.
TABLE I: Items for the HS-RCPS
- In the last month, I usually write my username and password on a
piece of paper and stick the paper onto my computer for easy
access
- In the last month, I sometimes visit at least one of the following
websites using the hospital’s computer: social media; Dropbox
and other public file storage systems; online music or videos sites;
online newspapers and magazines; personal e-mail accounts;
games; instant messaging services, etc
- In the last month, I did not often read the alert messages/emails
concerning security
- In the last month, I sometimes click on a link in an email from an
unknown sender
- In the last month, I usually postpone software updating activities
(restarting, clicking to run an update, accepting to update, or
following the update schedule) of my computers at my workplace
- In the last month, I usually postpone backup activities when I am
prompted
- In the last month, I usually do not prevent my colleagues from
seeing patients’ records for a non-therapeutic purpose when I am
working on patient information on my laptop
- In the last month, I did not post patient information on social
media
- In the last month, I sometimes share my passwords with my
colleagues in the hospital
- In the last month, I usually do not take any action when I notice
my colleague ignoring information security rules
- In the last month, I used a combination of letters, numbers, and
symbols in my work passwords
- In the last month, I have changed my passwords
Data Analysis
The present study employed SPSS software to analyze
the collected data. The reliability of the PSS and HS-RCPS
was measured using Cronbach’s alpha. Furthermore, Pearson’s
correlation coefficient was utilized to evaluate the relationship
between the PSS and HS-RCPS scales. The mean differences
among various demographic groups, such as age, position,
position level, and work experience, were assessed using
ANOVA. A t-test was utilized to evaluate the mean difference
in HS-RCPS scores between males and females. Additionally,
a Kruskal-Wallis test with Bonferroni-Dunn posthoc analysis
was conducted to examine the variance in HS-RCPS scores
among staff groups based on their country
Results
General characteristics of participants
In total, 389 hospital employees participated but 36 of them
failed to answer the attention-checking question correctly.
As seen in Table II, 353 qualified participants were finally
included in the study, with 212 participants from Ghana, 42 from Norway, and 99 from Indonesia. Based on gender, 209
(59.20%) of them are females and 143 of them are males
(40.50%). One participant (0.30%) preferred not to disclose
their gender. The age range of the participants varied, with 117
(33.10%) falling in the 21-31 years category, 168 (47.60%)
falling in the 31-40 years category, 47 (13.30%) falling in the
41-50 years category, and 21 (5.90%) falling in the over 50
years category. Regarding participants’ positions, 15 (4.20%)
were in top-level management, 34 (9.60%) were doctors, 180
(51.00%) were nurses, 22 (6.20%) were lab staff, 28 (7.90%) were pharmacy staff, 14 (4.00%) were IT staff, 3 (0.80%) were
researchers, 3 (0.80%) were nutritionists, and 54 (15.30%)
reported other positions. The participants’ position level was
categorized as executives (1.40%), managers and supervisors
(16.70%), and operational staff (81.90%). Regarding work
experience, 131 (37.10%) participants had less than six years
of experience, 166 (47.00%) had 6-15 years of experience, 46
(13.00%) had 16-25 years of experience, and 10 (2.80%) had
more than 25 years of experience.
TABLE II: Participant Characteristics
Variable Category n %
- Country:
- Ghana 212 60.10 %
- Norway 42 11.90 %
- Indonesia 99 28.00 %
- Gender
- Female 209 59.20 %
- Male 143 40.50 %
- Prefer not to say 1 0.30 %
- Age
- 21-31 117 33.10 %
- 31-40 168 47.60 %
- 41-50 47 13.30 %
- Over 50 21 5.90 %
- Position
- Top Level Management 15 4.20 %
- Doctor 34 9.60 %
- Nurse 180 51.00 %
- Lab staff 22 6.20 %
- Pharmacy staff 28 7.90 %
- IT staff 14 4.00 %
- Researcher 3 0.80 %
- Nutritionist 3 0.80 %
- Other 54 15.30 %
- Position level Executive 5 1.40 %
- Managers and supervisors 59 16.70 %
- Operational staff 289 81.90 %
- Work experience
- <6 Year 131 37.10 %
- 6-15 Years 166 47.00 %
- 16-25 Years 46 13.00 %
- >25 Years 10 2.80 %
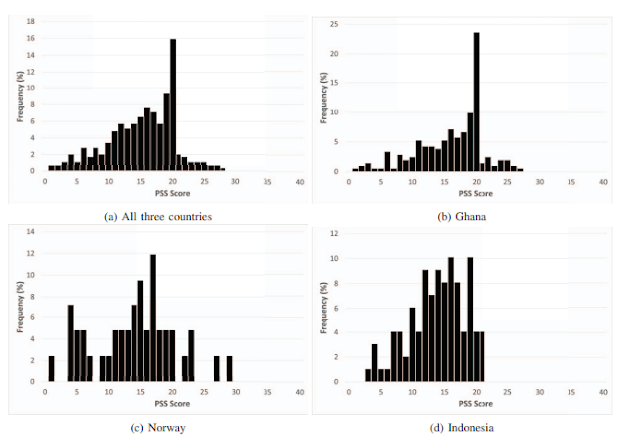
PSS Score
Figure 2 displays the distribution of Perceived Stress Scale
(PSS) scores among the study participants. The PSS is a selfreported scale that measures the degree to which individuals
perceive their lives as stressful. The scores range from 0 to
40, with higher scores indicating higher levels of perceived
stress during the past month. The statistic of the PSS score
from the three countries is depicted in table III. Ghana had the
highest PSS score average, followed by Norway, and Indonesia
became the last. From Ghana, the PSS scores reported ranged
from 1 to 27, with an average score of 16.12 and a standard
deviation of 5.23. The lowest PSS score was obtained by one
participant with 1, while the highest score was also reported
by one participant with 27. From Norway, the PSS scores
reported ranged from 1 to 29, with an average score of 14.05
and a standard deviation of 6.4. The lowest PSS score was
obtained by one staff member, while the highest score was
also reported by one staff member. From Indonesia, the PSS
scores reported ranged from 3 to 21, with an average score
of 13.89 and a standard deviation of 4.41. The lowest PSS
score was obtained by one participant, while the highest score
was reported by four participants. Combining all of the results from these three countries, the mean PSS score was 15.25 with
a standard deviation of 5.28.
Finally, we assessed the reliability of the PSS. According to
the survey results, PSS in English, Norwegian, and Indonesian
versions had Cronbach’s α of 0.750, 0.844, and 0.733, respectively. It indicates that the items in all three PSS versions had
a good level of internal consistency [18], [19].
Figure 2: Frequency distribution of the PSS score:
TABLE III: Descriptive statistic of PSS score in Ghana,
Norway, and Indonesia
TABLE IV: Descriptive statistic of HS-RCPS score in Ghana,
Norway, and Indonesia.
TABLE V: Descriptive statistic of risky cybersecurity practices
score based on gender
TABLE VI: Descriptive statistic of risky cybersecurity practices score based on age.
The distribution and statistics of the HS-RCPS scores are
shown in Figure 3 and Table IV. HS-RCPS is a scale of 0 to
48, with 0 denoting the lowest risky cybersecurity practice
and 48 denoting the highest. Overall, the results showed
that the mean HS-RCPS score for all three countries was
14.94, with a standard deviation of 6.64. From Ghana, the
results indicate that the minimum HS-RCPS score among the
participants was 0, while the maximum was 36. The mean
score was 15.95 with a standard deviation of 6.64. Meanwhile,
the minimum and maximum scores in Norway were 2 and 26,
respectively, with a mean of 10.88 and a standard deviation
of 4.90. Finally, in Indonesia, the minimum and maximum
scores were 0 and 27, respectively, with a mean of 14.49
and a standard deviation of 6.64. The findings suggest that
risky cybersecurity practice is relatively low among individuals
in the three countries. Comparatively, Ghana had the highest
mean score while Norway had the lowest.
Furthermore, the reliability of the HS-RCPS was assessed
through survey results obtained from Ghana, Norway, and
Indonesia. The scale’s internal consistency was evaluated using
Cronbach’s α coefficient. The survey results from Ghana, Norway, and Indonesia indicated that the scale had a Cronbach’s
α of 0.595, 0.502, and 0.697, respectively. Overall, the HSRCPS demonstrated acceptable internal consistency across the
surveyed populations [18]–[20].
Demographic and Risky Cybersecurity Practices
The descriptive statistic of risky cybersecurity practices
score based on gender, age, position, position level, and work
experience are displayed in Table V, VI, VII, VIII, and IX
respectively. The statistical analysis revealed no significant differences in the levels of risky cybersecurity practices between male and female participants. Technically, the t-test results
indicated that the mean scores for females (M = 14.65, SD =
6.47) and males (M = 15.32, SD = 6.90) were not significantly
different, t(350) = 0.980, p = 0.323. In addition, the ANOVA
results indicated that there were no significant differences in
mean scores of risky cybersecurity practices among various
groups, including age (F(3, 349) = 0.347, p = 0.791), position
(F(8, 344) = 1.774, p = 0.081), position level (F(2, 350) =
0.144, p = 0.866), and work experience (F(3, 349) = 1.369, p
= 0.252).
On the other hand, the Kruskal-Wallis test showed that the
scores for risky cybersecurity practices varied significantly
across various staff groups based on country (χ2(2) = 23.124,
p < 0.001). Specifically, the scores for hospital staff from
Norway were significantly lower than those from Ghana and
Indonesia (p = 0.000 and p=0.04, respectively), suggesting that
hospital staff from Norway have better cybersecurity practices.
Correlation Between Stress Level and Cybersecurity Practices
Table X presents the correlation between the perceived
stress levels of hospital staff and their risky cybersecurity
practices. The results reveal that there was a statistically
significant positive correlation between staff’s stress levels and their cybersecurity practices, as indicated by a Pearson’s
correlation coefficient of r = 0.201 (p < 0.01). This finding
suggests that employees who reported higher levels of stress,
as measured by the Perceived Stress Scale (PSS), were also
more likely to engage in riskier cybersecurity practices, as
assessed by the Hospital Staff Risky Cybersecurity Practices
Scale (HS-RCPS). Specifically, item 4 of the HS-RCPS, which
measures staff’s tendency to click on links from unknown
sources, had the highest positive correlation with stress levels,
indicating that this is the riskiest cybersecurity behavior that
is most influenced by stress levels among hospital staff. In
addition, this significant correlation also appears when we
analyze only the data from Ghana or only the data from
Indonesia with r = 0.138 (p < 0.05) and r = 0.311 (p < 0.01),
respectively. However, a significant correlation between stress
and risky cybersecurity practices was not found in Norway (r
= 0.101).
TABLE VII: Descriptive statistic of risky cybersecurity practices score based on position.
TABLE VIII: Descriptive statistic of risky cybersecurity practices score based on position level.
TABLE IX: Descriptive statistic of risky cybersecurity practices score based on years of work experience
TABLE X: PSS score correlation to cybersecurity practices
score.
The results of this study have important implications for
organizations concerned with cybersecurity and employee
well-being. The positive correlation between stress levels and
risky cybersecurity practices supports the notion that stress
can impair cognitive functioning and increase the likelihood
of individuals engaging in risky behavior, including online behavior. This is consistent with the broader literature on the
negative effects of stress on decision-making [11], [12]. This
result was also supported by Fauzi et al. [21] and McCormac
et al. [13] who found that workers with greater levels of
stress engaged in riskier cybersecurity practices or had worse
information security awareness (ISA).
From a practical perspective, these findings highlight the
importance of addressing stress and well-being in the context
of cybersecurity training and awareness programs. Specifically,
organizations should consider incorporating stress management techniques and well-being training into their cybersecurity training programs to help employees manage stress and reduce their engagement in risky cybersecurity practices. Having
an understanding of how stress can influence an individual’s
cybersecurity practices, one can take measures to regulate
their stress levels and maintain a heightened awareness of
their cybersecurity practices. These measures could comprise
tactics such as taking breaks to alleviate stress, exercising
increased mindfulness with regard to cybersecurity practices
while experiencing stress, and seeking assistance as necessary.
Furthermore, the finding that clicking on links from unknown sources was the riskiest cybersecurity behavior most
influenced by stress levels is also reasonable since stress can
harm an individual’s cognitive functioning, impairing their
ability to make rational decisions and increasing the likelihood
of impulsive behavior [10]. In addition, stress can lead to feelings of anxiety or overwhelm, causing individuals to rush
through tasks or pay less attention to details, making them
more likely to overlook the signs of a phishing email [22].
In addition, the research results also revealed a significant
difference in cybersecurity practices between healthcare professionals in Norway, a developed country, and those in Ghana
and Indonesia, two developing countries. Developing nations
have historically slowly adopted and utilized computer and
internet technologies. As identified by Ben-David et al.’s research [23], developing nations’ security landscape is affected
by five fundamental factors: inadequate ”security hygiene,”
unique resource constraints (such as one computer for multiple
users), novice internet users, use of pirated software, and
limited comprehension of cybersecurity adversaries. These
factors could explain why people in developing countries
generally exhibit poorer cybersecurity practices than their
counterparts in developed nations. Insufficient IT education
and a lack of computer and internet manuals in local languages
have also contributed to unsafe cybersecurity practices [24].
Moreover, Norway’s healthcare systems and infrastructure are
comparatively advanced and better equipped to implement and
enforce cybersecurity protocols than Indonesia and Ghana.
Future research can investigate cultural factors and explore
how they may be leveraged to improve cybersecurity practices
in different regions.
Limitations
There are several limitations of this study that need to
be acknowledged. First, the study used a self-report survey
to collect data, which may result in social desirability bias,
meaning that participants may have needed to be more honest
in their responses. Second, memory bias could also occur
when participants have trouble remembering details correctly,
particularly if the details relate to previous events or behaviors.
Finally, the study’s cross-sectional design precludes the establishment of causality. Using this study design, it is difficult
to determine if high-stress levels cause risky cybersecurity
practices or if it is the other way around.
Conclussions
In conclusion, this study explored the relationship between
stress levels and risky cybersecurity practices among hospital
staff in three countries. The results showed a statistically
significant positive correlation between staff stress levels and
their engagement in riskier cybersecurity practices. Specifically, the staff’s tendency to click on links from unknown
sources was found to be the risky cybersecurity practice
most heavily associated with higher stress levels. Interestingly,
no significant differences were found in the levels of risky
cybersecurity practices between male and female participants
or among different age groups, positions, position levels,
and work experience. However, a significant difference was
observed in risky cybersecurity practices scores across staff
groups based on the country of origin, with hospital staff from
Norway showing significantly lower scores than those from
Ghana and Indonesia, suggesting Norwegian healthcare staff
had safer cybersecurity practices.
There are several directions that future studies can take
based on the findings of this study. Firstly, further research
can explore the causal relationship between stress levels and
cybersecurity practices. Second, future studies can explore
other factors influencing risky cybersecurity practices among
hospital staff, such as personality traits, motivation, or job
satisfaction. By gaining a more comprehensive understanding
of the various factors that influence cybersecurity practices,
interventions can be developed that target these factors to
promote safer cybersecurity behaviors among employees. Finally, future studies can examine the effectiveness of various
interventions aimed at promoting safer cybersecurity practices
among hospital staff. Such interventions may include training
programs, awareness campaigns, or technological solutions
such as secure communication platforms.
References
[1] Verizon, “2022 data breach investigations report,” Available online:
https://enterprise.verizon.com/resources/reports/dbir (accessed on 18
March 2023), 2022.
[2] E. D. Perakslis, “Cybersecurity in health care,” N Engl J Med, vol. 371,
no. 5, pp. 395–397, 2014.
[3] M. Warkentin and R. Willison, “Behavioral and policy issues in information systems security: the insider threat,” European Journal of
Information Systems, vol. 18, no. 2, pp. 101–105, 2009.
[4] Z. Yan, T. Robertson, R. Yan, S. Y. Park, S. Bordoff, Q. Chen, and
E. Sprissler, “Finding the weakest links in the weakest link: How well
do undergraduate students make cybersecurity judgment?” Computers
in Human Behavior, vol. 84, pp. 375–382, 2018.
[5] M. Whitty, J. Doodson, S. Creese, and D. Hodges, “Individual differences in cyber security behaviors: an examination of who is sharing
passwords,” Cyberpsychology, Behavior, and Social Networking, vol. 18,
no. 1, pp. 3–7, 2015.
[6] T. Halevi, N. Memon, J. Lewis, P. Kumaraguru, S. Arora, N. Dagar,
F. Aloul, and J. Chen, “Cultural and psychological factors in cybersecurity,” in Proceedings of the 18th International Conference on
Information Integration and Web-based Applications and Services, 2016,
pp. 318–324.
[7] M. Gratian, S. Bandi, M. Cukier, J. Dykstra, and A. Ginther, “Correlating
human traits and cyber security behavior intentions,” computers &
security, vol. 73, pp. 345–358, 2018.
[8] P. K. Yeng, B. Yang, and E. A. Snekkenes, “Framework for healthcare
security practice analysis, modeling and incentivization,” in 2019 IEEE
International Conference on Big Data (Big Data). IEEE, 2019, pp.
3242–3251.
[9] S. M. Kennison and E. Chan-Tin, “Taking risks with cybersecurity:
Using knowledge and personal characteristics to predict self-reported
cybersecurity behaviors,” Frontiers in Psychology, vol. 11, p. 3030,
2020.
[10] L. Simon, T. Jiryis, and R. Admon, “Now or later? stress-induced
increase and decrease in choice impulsivity are both associated with
elevated affective and endocrine responses,” Brain Sciences, vol. 11,
no. 9, p. 1148, 2021.
[11] E. Michailidis and A. P. Banks, “The relationship between burnout and
risk-taking in workplace decision-making and decision-making style,”
Work & Stress, vol. 30, no. 3, pp. 278–292, 2016.
[12] S. E. Wemm and E. Wulfert, “Effects of acute stress on decision
making,” Applied psychophysiology and biofeedback, vol. 42, no. 1, pp.
1–12, 2017.
[13] A. McCormac, D. Calic, K. Parsons, M. Butavicius, M. Pattinson, and
M. Lillie, “The effect of resilience and job stress on information security
awareness,” Information & Computer Security, 2018.
[14] T. Fordyce, S. Green, and T. Groß, “Investigation of the effect of fear
and stress on password choice,” in Proceedings of the 7th Workshop on
Socio-Technical Aspects in Security and Trust, 2018, pp. 3–15.
[15] S. Cohen, T. Kamarck, and R. Mermelstein, “Perceived stress scale
(pss),” J Health Soc Beh, vol. 24, p. 285, 1983.
[16] T. L. Pin, “Hubungan kebiasaan berolahraga dengan tingkat stres pada
mahasiswa fakultas kedokteran universitas sumatera utara tahun masuk 2008,” Skripsi. Medan: Fakultas Kedokteran Universitas Sumatera
Utara, 2011.
[17] C. M. U. Department of Psychology. (2015, Feb.) Scales -
laboratory for the study of stress, immunity, and disease.
[Online]. Available: https://www.cmu.edu/dietrich/psychology/stressimmunity-disease-lab/scales/index.html
[18] K. S. Taber, “The use of cronbach’s alpha when developing and reporting research instruments in science education,” Research in Science
Education, vol. 48, no. 6, pp. 1273–1296, 2018.
[19] M. S. B. Yusoff, “Stability of dreem in a sample of medical students: a
prospective study,” Education Research International, vol. 2012, 2012.
[20] R. Berger and M. Hanze, “Impact of expert teaching quality on novice ¨
academic performance in the jigsaw cooperative learning method,”
International Journal of Science Education, vol. 37, no. 2, pp. 294–
320, 2015.
[21] M. A. Fauzi, P. Yeng, B. Yang, and D. Rachmayani, “Examining the
link between stress level and cybersecurity practices of hospital staff
in indonesia,” in Proceedings of the 16th International Conference on
Availability, Reliability and Security, 2021, pp. 1–8.
[22] Q. Liu, Y. Liu, X. Leng, J. Han, F. Xia, and H. Chen, “Impact of chronic
stress on attention control: Evidence from behavioral and event-related
potential analyses,” Neuroscience bulletin, vol. 36, pp. 1395–1410, 2020.
[23] Y. Ben-David, S. Hasan, J. Pal, M. Vallentin, S. Panjwani, P. Gutheim,
J. Chen, and E. A. Brewer, “Computing security in the developing world:
A case for multidisciplinary research,” in Proceedings of the 5th ACM
workshop on Networked systems for developing regions, 2011, pp. 39–
44.
[24] M. Grobler and J. J. van Vuuren, “Broadband broadens scope for cyber
crime in africa,” in 2010 Information Security for South Africa. IEEE,
2010, pp. 1–8.









Comments
Post a Comment